By: patricia cartwright
Overview
In my blog, I will discuss social neuroscience research findings regarding the processing of social pain. Social pain is the result of events that include social exclusion from groups or activities, being dismissed, ignored, bullied, the death of a loved one, and the loss of a romantic partner. Together, these findings help us understand the consequences of rejection are grave and can lead others to engage in attempts to affiliate (e.g., through conformity), withdraw, and become aggressive. Lastly, the social neuroscience literature findings have implications for how we should respond when social pain occurs and the steps that should be taken to prevent a toll being taken on psychological and physical health in those who encounter more frequent social pain.
Evolutionary Advantages of Social Pain
According to social neuroscience research, physical and social pain activate similar brain circuits such as the anterior cingulate cortex. The anterior cingulate cortex is responsible for the ability to control and regulate painful emotions (Stevens et al. 2011). Human beings are social animals that experience happiness and a sense of quality of life, often times, when their interpersonal relationships are healthy, intimate, and satisfying. From an evolutionary perspective, humans developed the ability to pass on characteristics that have survival and fitness value, such as relationships and social bonds. The existence of intimate relationships, group cohesion, and social bonds increases our odds to survive and reproduce in contrast to social exclusion. Thus, the brain activates a neural pain system in the brain for both physical and social pain to promote survival.
Social Pain Arousal
Social exclusion threatens the need to feel connected to others, the need to have control over one’s environment, the need for self-value and self-respect, and the sense of purpose and meaning. When people face social pain through events such as social exclusion, people experience negative emotions that can be crippling. Research has also found that people experience physiological arousal and stress responses (e.g., increases in cortisol and decreases in norepinephrine), creating the perception of physical pain, when they are socially excluded from a group activity. Thus, social pain is allegedly processed similar to physical pain.
Brain Representations for Pain and Rejection
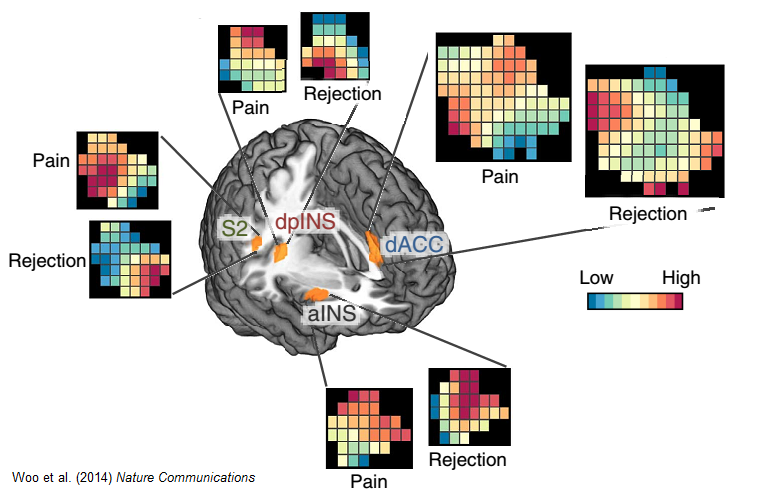
Whereas some researchers have found that when individuals experience social exclusion in a simulated social exclusion activity, the brain regions associated with the experience and regulation of pain distress are activated (Eisenberger, Lieberman, & Williams, 2003) other research has found conflicting results. Woo et al. (2014) identified neuroimaging patterns that are sensitive and specific to social pain and physical pain within core pain-processing brain regions. This evidence conflicts with the shared representation theory of social pain because although social and physical pain engage the same areas of the brain they are processed in different ways within those areas as shown in the image below (Rogachov, Cheng, DeSouza, 2015). However, one important limitation of the Woo et al. (2014) study was the use of past experiences of social pain where participants had to relive pain, instead of having participants experience pain in the current moment. Therefore, caution must be exerted when interpreting these findings since memory processes must have also been employed. Nevertheless, the pattern of neural activity for social pain holds important implications for how we understand the behavioral consequences of rejection that the multimotive theory helps explain.
The Multimotive Theory
Richman & Leary (2009) proposed that individuals experience three sets of motives, which may arise simultaneously, after they experience social rejection. These motives include an increase in the desire for social connectedness (i.e., seeking acceptance and support), antisocial urges tinged with anger (i.e., seeking to defend oneself or hurt others), and avoidance and withdrawal (i.e., people withdraw to avoid future rejection and emotional pain). Furthermore, the multimotive theory seeks to explain which of the three motives will guide one’s behavior based off of how people construe the rejection and the level of fairness involved, expectations for relationship repair, pervasiveness of the rejection, and the possibility of alternatives (Richman & Leary, 2009). The multimotive theory further postulates that people’s perceptions of the social rejection can predict which motive prevails at a certain time as well as long-term physical and mental health outcomes.
Psychological & Physical Consequences of Rejection
Events that involve rejection typically result in the immediate response of negative affect and lowered self-esteem (Richman & Leary, 2009). People typically describe the negative affect they experience as hurt feelings (e.g., sadness, anxiety, grief, anger, and confusion). Additionally, social isolation has also been shown to affect gene expression that can increase one’s risk for heart attacks, metastatic cancer, Alzheimer’s, and other illnesses. Researchers have found that immune system responses in isolated individuals are compromised, meaning the antibodies in the human body that function to fight off infections are weakened and inflammation is increased. Chronic loneliness has also been found to contribute to chronic immune system impairment and health-care utilization. In light of the psychological and physical consequences of rejection, the next question we wish to answer is what are the implications for clinical and medical practices.
Significance of Findings
Given that social neuroscience research demonstrates there are significant overlaps in how the brain processes physical and social pain, they should no longer be considered in isolation by healthcare professionals. Instead, healthcare professionals should consider social pain to be a serious ailment and treatment and interventions should be employed to alleviate social pain just as commonly as physical pain. For instance, treatment providers should provide individuals with information and resources about social groups in their area that offer social support, a sense of belonging, opportunities for social activities, etc. Furthermore, treatments and interventions should emphasize behavioral changes to combat social rejection, loneliness, and other forms of social pain as it is closely tied to poor psychological and physical health outcomes. Moreover, national campaigns should be used to highlight the implications of loneliness and social rejection on both psychological and physical health to raise public awareness.
References
Eisenberger, N. I., Lieberman, M. D. & Williams, K. D. (2003). Does rejection hurt? An fMRI study of social exclusion. American Association for the Advancement of Science, 302, 290-292.
Rogachov, A., Cheng, J. C., & DeSouza, D. D. (2015). Discriminating neural representations of physical and social pains: how multivariate statistics challenge the “shared representation” theory of pain. Journal of Neurophysiology, 114(5), 2558–2560. http://doi.org/10.1152/jn.00075.2015
Richman, L. S., & Leary, M. R. (2009). Reactions to discrimination, stigmatization, ostracism, and other forms of interpersonal rejection: A multimotive model. Psychological Review, 116(2), 365–383. http://doi.org/10.1037/a0015250
Stevens, F. L., Hurley, R. A., Taber, K. H., Hurley, R. A., Hayman, L. A., & Taber, K. H. (2011). Anterior cingulate cortex: Unique role in cognition and emotion. The Journal of Neuropsychiatry and Clinical Neurosciences, 23, 121-125.
Woo, C.-W. et al. (2014). Separate neural representations for physical pain and social rejection. Nature Communications, 5, 5380. http://doi.org/10.1038/ncomms6380
In my blog, I will discuss social neuroscience research findings regarding the processing of social pain. Social pain is the result of events that include social exclusion from groups or activities, being dismissed, ignored, bullied, the death of a loved one, and the loss of a romantic partner. Together, these findings help us understand the consequences of rejection are grave and can lead others to engage in attempts to affiliate (e.g., through conformity), withdraw, and become aggressive. Lastly, the social neuroscience literature findings have implications for how we should respond when social pain occurs and the steps that should be taken to prevent a toll being taken on psychological and physical health in those who encounter more frequent social pain.
Evolutionary Advantages of Social Pain
According to social neuroscience research, physical and social pain activate similar brain circuits such as the anterior cingulate cortex. The anterior cingulate cortex is responsible for the ability to control and regulate painful emotions (Stevens et al. 2011). Human beings are social animals that experience happiness and a sense of quality of life, often times, when their interpersonal relationships are healthy, intimate, and satisfying. From an evolutionary perspective, humans developed the ability to pass on characteristics that have survival and fitness value, such as relationships and social bonds. The existence of intimate relationships, group cohesion, and social bonds increases our odds to survive and reproduce in contrast to social exclusion. Thus, the brain activates a neural pain system in the brain for both physical and social pain to promote survival.
Social Pain Arousal
Social exclusion threatens the need to feel connected to others, the need to have control over one’s environment, the need for self-value and self-respect, and the sense of purpose and meaning. When people face social pain through events such as social exclusion, people experience negative emotions that can be crippling. Research has also found that people experience physiological arousal and stress responses (e.g., increases in cortisol and decreases in norepinephrine), creating the perception of physical pain, when they are socially excluded from a group activity. Thus, social pain is allegedly processed similar to physical pain.
Brain Representations for Pain and Rejection
Whereas some researchers have found that when individuals experience social exclusion in a simulated social exclusion activity, the brain regions associated with the experience and regulation of pain distress are activated (Eisenberger, Lieberman, & Williams, 2003) other research has found conflicting results. Woo et al. (2014) identified neuroimaging patterns that are sensitive and specific to social pain and physical pain within core pain-processing brain regions. This evidence conflicts with the shared representation theory of social pain because although social and physical pain engage the same areas of the brain they are processed in different ways within those areas as shown in the image below (Rogachov, Cheng, DeSouza, 2015). However, one important limitation of the Woo et al. (2014) study was the use of past experiences of social pain where participants had to relive pain, instead of having participants experience pain in the current moment. Therefore, caution must be exerted when interpreting these findings since memory processes must have also been employed. Nevertheless, the pattern of neural activity for social pain holds important implications for how we understand the behavioral consequences of rejection that the multimotive theory helps explain.
The Multimotive Theory
Richman & Leary (2009) proposed that individuals experience three sets of motives, which may arise simultaneously, after they experience social rejection. These motives include an increase in the desire for social connectedness (i.e., seeking acceptance and support), antisocial urges tinged with anger (i.e., seeking to defend oneself or hurt others), and avoidance and withdrawal (i.e., people withdraw to avoid future rejection and emotional pain). Furthermore, the multimotive theory seeks to explain which of the three motives will guide one’s behavior based off of how people construe the rejection and the level of fairness involved, expectations for relationship repair, pervasiveness of the rejection, and the possibility of alternatives (Richman & Leary, 2009). The multimotive theory further postulates that people’s perceptions of the social rejection can predict which motive prevails at a certain time as well as long-term physical and mental health outcomes.
Psychological & Physical Consequences of Rejection
Events that involve rejection typically result in the immediate response of negative affect and lowered self-esteem (Richman & Leary, 2009). People typically describe the negative affect they experience as hurt feelings (e.g., sadness, anxiety, grief, anger, and confusion). Additionally, social isolation has also been shown to affect gene expression that can increase one’s risk for heart attacks, metastatic cancer, Alzheimer’s, and other illnesses. Researchers have found that immune system responses in isolated individuals are compromised, meaning the antibodies in the human body that function to fight off infections are weakened and inflammation is increased. Chronic loneliness has also been found to contribute to chronic immune system impairment and health-care utilization. In light of the psychological and physical consequences of rejection, the next question we wish to answer is what are the implications for clinical and medical practices.
Significance of Findings
Given that social neuroscience research demonstrates there are significant overlaps in how the brain processes physical and social pain, they should no longer be considered in isolation by healthcare professionals. Instead, healthcare professionals should consider social pain to be a serious ailment and treatment and interventions should be employed to alleviate social pain just as commonly as physical pain. For instance, treatment providers should provide individuals with information and resources about social groups in their area that offer social support, a sense of belonging, opportunities for social activities, etc. Furthermore, treatments and interventions should emphasize behavioral changes to combat social rejection, loneliness, and other forms of social pain as it is closely tied to poor psychological and physical health outcomes. Moreover, national campaigns should be used to highlight the implications of loneliness and social rejection on both psychological and physical health to raise public awareness.
References
Eisenberger, N. I., Lieberman, M. D. & Williams, K. D. (2003). Does rejection hurt? An fMRI study of social exclusion. American Association for the Advancement of Science, 302, 290-292.
Rogachov, A., Cheng, J. C., & DeSouza, D. D. (2015). Discriminating neural representations of physical and social pains: how multivariate statistics challenge the “shared representation” theory of pain. Journal of Neurophysiology, 114(5), 2558–2560. http://doi.org/10.1152/jn.00075.2015
Richman, L. S., & Leary, M. R. (2009). Reactions to discrimination, stigmatization, ostracism, and other forms of interpersonal rejection: A multimotive model. Psychological Review, 116(2), 365–383. http://doi.org/10.1037/a0015250
Stevens, F. L., Hurley, R. A., Taber, K. H., Hurley, R. A., Hayman, L. A., & Taber, K. H. (2011). Anterior cingulate cortex: Unique role in cognition and emotion. The Journal of Neuropsychiatry and Clinical Neurosciences, 23, 121-125.
Woo, C.-W. et al. (2014). Separate neural representations for physical pain and social rejection. Nature Communications, 5, 5380. http://doi.org/10.1038/ncomms6380
 RSS Feed
RSS Feed
